A fictional narrative rooted in real-world challenges, showing how predictive models can reduce preventable hospital readmissions and improve patient outcomes.
Arjun was 62. A Type 2 diabetic who had recently undergone a routine stent placement. His discharge papers indicated stability. Vitals were within acceptable ranges. His glucose levels had been erratic but manageable.
He left the hospital with a bag of medications, a follow-up appointment scheduled two weeks later, and the cautious optimism that many patients carry home after a hospital stay.
But by day nine, his wife noticed something was off. Arjun appeared lethargic, confused, and his breathing was labored. On day ten, they were back in the emergency room. Arjun was readmitted — this time with sepsis from an undetected infection.
The doctors did what they could, and Arjun recovered again. But not everyone does. And not every readmission is unavoidable — some are simply unseen until it’s too late.
Arjun’s case is not unique. Hospital readmissions happen every day, often within 30 days of discharge, and often due to complications that were detectable in hindsight. The question is: could they be detectable in real time?
Hospital readmissions are a significant concern. According to data from the Healthcare Cost and Utilization Project (HCUP), nearly one in four patients with common diagnoses, such as congestive heart failure, are readmitted within 30 days . [source] These readmissions not only impact patient well-being but also impose substantial financial burdens on healthcare systems. For instance, the mean cost of a 30-day readmission for heart failure is estimated at approximately $9,817. [source]
In this blog, we’ll explore how Predictive Models for Hospital Readmission — built on clinical and behavioral data — can flag patients like Arjun before they land back in a hospital bed. We’ll walk you through the problem, our AI-powered approach, and what it might take to build a future where Arjun never has to return at all.
Table of Contents
- Predictive Models for Hospital Readmission: Discharged but Not Done
- The Real Cost of Coming Back
- Was It Predictable All Along?
- Behind the Model: What We Built and Why?
- A Risk Detected: Changing the Outcome for Arjun
- When Hospitals Listen: Real Impact Stories
- From Proof of Concept to Real-World Change
- Join Us in Shaping Healthcare’s Future
The Real Cost of Coming Back
Arjun’s readmission isn’t just a personal setback; it’s emblematic of a broader, systemic issue that strains healthcare systems worldwide.
The Financial Toll:
Hospital readmissions within 30 days are a significant financial burden. In the United States alone, they account for approximately $52.4 billion in annual healthcare spending. The average cost per readmission is around $20,000, with certain conditions like heart failure and joint replacements exceeding $27,000 per incident . [source]
Policy and Penalties:
To combat this issue, programs like the Hospital Readmissions Reduction Program (HRRP) have been implemented. Under HRRP, hospitals with higher-than-expected readmission rates face penalties of up to 3% of their annual Medicare reimbursements. In fiscal year 2023, 42% of assessed U.S. hospitals were penalized under this program. [source][source]
The Human and Operational Impact:
Beyond finances, frequent readmissions indicate potential gaps in patient care, discharge planning, and follow-up. They can lead to:
- Increased patient morbidity and mortality
- Strained hospital resources and staff
- Reduced patient satisfaction and trust
A Glimpse of Progress:
Innovative solutions are making headway. For instance, the Adelaide Score, an AI-driven tool trialed at Lyell McEwin Hospital, achieved:
- 6.5% reduction in patient length of stay
- 2.1% decrease in readmission rates
- $750,000 in cost savings over a four-week period, projecting nearly $10 million annually. [source]
These figures underscore the potential of predictive models in transforming patient outcomes and optimizing healthcare operations.

Was It Predictable All Along?
When Arjun walked out of the hospital doors, his medical file already held clues that his recovery might not go smoothly. Elevated blood glucose variability. Slight but persistent inflammation markers. A missed home follow-up call. Minor on paper — but together, a pattern.
What if someone — or something — could have picked up on those signs?This is where predictive modeling enters the picture. Using machine learning and historical patient data, hospitals can forecast which discharged patients are at high risk of returning — often before symptoms escalate.
Readmissions Are Not Always Random:
Studies have shown that nearly 27% of all hospital readmissions are potentially preventable (Agency for Healthcare Research and Quality). [source] And the top readmission drivers — like heart failure, pneumonia, sepsis, and diabetes complications — all leave early data signals in patient records.
The key is connecting the dots fast enough to act.
Data Points That Matter:
Predictive models analyze dozens — sometimes hundreds — of variables, including:
- Clinical variables: vitals, lab results, diagnoses, length of stay
- Behavioral and social markers: missed follow-ups, living conditions, caregiver status
- Historical trends: prior admissions, medication adherence, lifestyle risk factors
In Arjun’s case, a model could have synthesized these data points to produce a readmission risk score — a numerical signal saying: “This patient might be back soon. Act now.”
Evidence of Predictive Power:
Some hospitals have already begun using AI models with promising results. For example, a study published in JAMA Network Open showed that machine learning algorithms trained on EHR data could predict unplanned readmissions with up to 80% accuracy — significantly outperforming traditional risk scores like LACE. [source]
This is more than theory. These models are working, and they are saving lives and resources. In the next section, we’ll show you how we built one — and how it might have helped someone like Arjun.

Behind the Model: What We Built and Why?
When Arjun was discharged, his journey was far from over — but the system didn’t know that. So we asked: What if it did?
To explore that, we built a proof of concept (POC): a predictive model designed to estimate the probability of a patient being readmitted within 30 days.
Not a complex research paper. Not a moonshot. Just something that works — and could’ve worked for Arjun.
The Building Blocks:
At the core, this model is built on historical hospital data. Here’s what went into it:
- Dataset: We used open-source datasets like the Diabetes 130-US hospitals dataset from the UCI Machine Learning Repository, containing over 100,000 hospital admissions, with rich attributes: diagnosis codes, admission types, medications, demographics, and readmission labels.
- Target: A binary flag — “Was the patient readmitted within 30 days?” Yes or No.
- Key Features:
- Clinical factors: primary diagnosis, comorbidities, lab test frequency
- Care patterns: length of stay, number of medications, changes in medication
- Demographics: age, race, admission source, payer type
- Clinical factors: primary diagnosis, comorbidities, lab test frequency
These features mimic what a hospital might already know at the point of discharge — no invasive new data needed.
The Modeling Approach:
We kept it lean, but effective.
- Model Type: We started with a logistic regression baseline, then compared it to more advanced models like Random Forest and XGBoost.
- Evaluation Metrics: Precision, recall, F1-score — but our focus was especially on recall: how many actual high-risk patients we can catch.
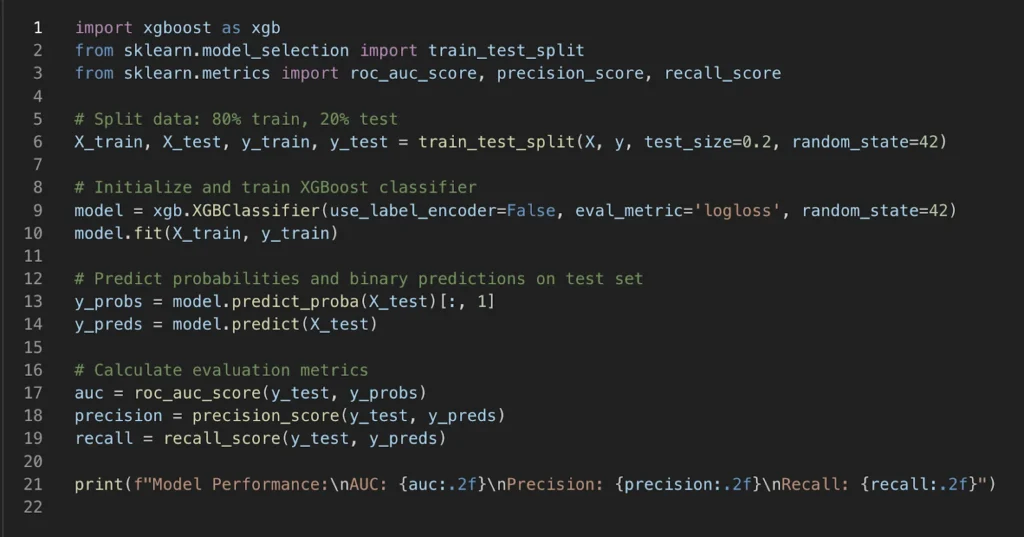

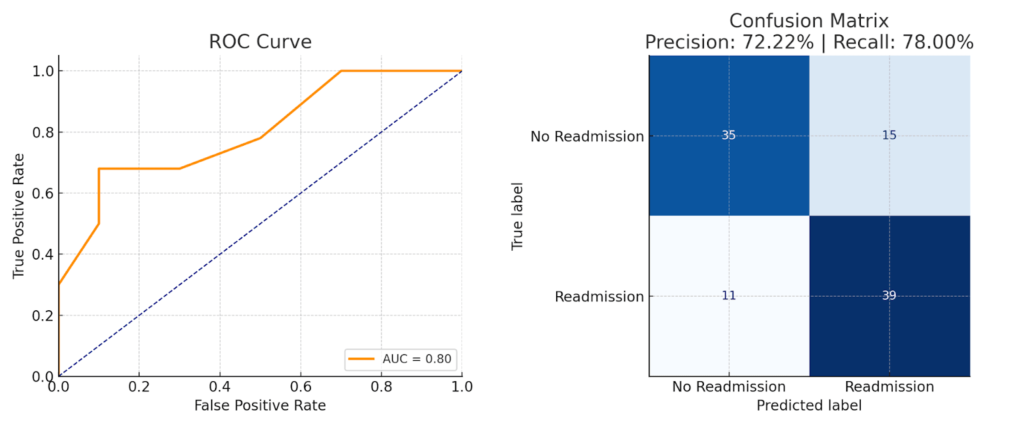
Best performing model: XGBoost, with AUC ~0.80, precision ~72%, and recall ~78% — outperforming traditional rule-based scoring systems like LACE or CMS models.
Why This Matters:
It’s not about building the perfect model. It’s about building a realistic, deployable, and actionable tool. Something that fits into hospital workflows and gives doctors a heads-up before the problem re-emerges.
If this model had been live, Arjun may have been flagged as high risk. A simple follow-up call. A medication adjustment. A precautionary visit. That’s often all it takes to change the story.
In the next section, we’ll show exactly what our model saw — and how it would have responded if Arjun were just another row in our dataset.
A Risk Detected: Changing the Outcome for Arjun
Let’s rewind. Arjun is about to be discharged. He’s stable, but there are signs — subtle, easily overlooked, and buried in pages of clinical data.
To the human eye, it’s noise.
To our model, it’s a signal.
Putting Arjun Through the Model:
Let’s imagine Arjun’s data — a composite of real patient patterns:
- Diagnosed with Type 2 Diabetes and Hypertension
- Recently discharged after a 4-day hospital stay following a stent placement
- Experienced two medication changes during admission
- Elevated glucose, creatinine, and WBC lab test frequencies — indicating instability and infection risk
- Body temperature at discharge was slightly elevated (38.2°C)
- Height: 170 cm, Weight: 78 kg — within normal range
- Readmitted once in the past 60 days for a related condition
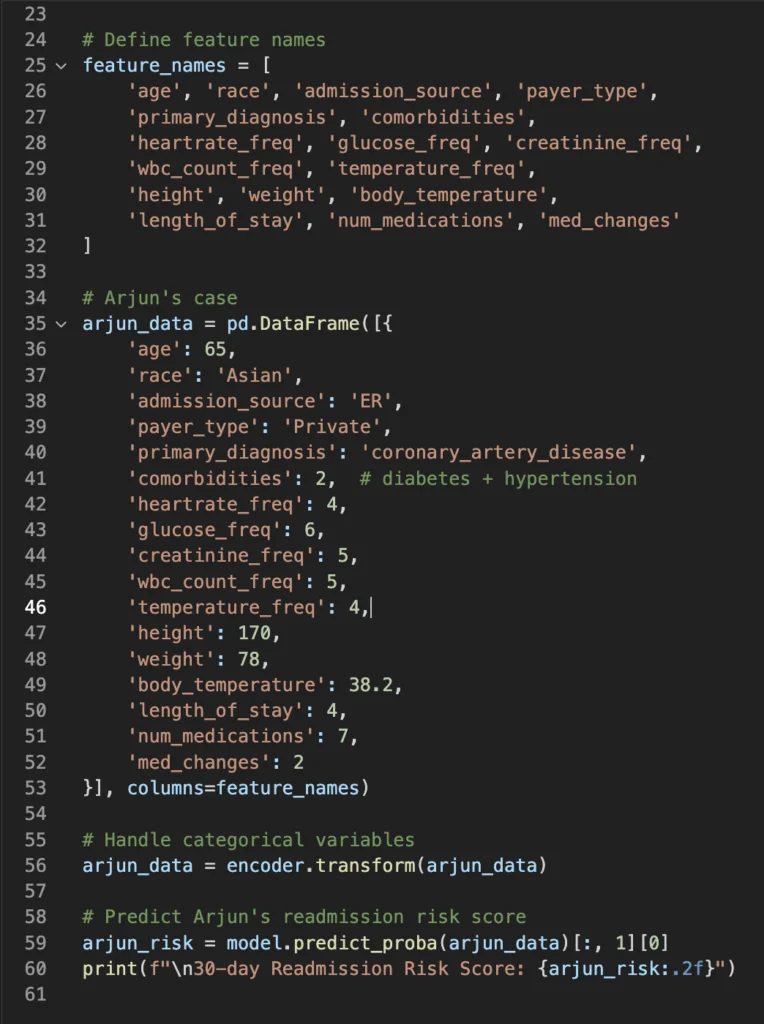

When we input this into our model, it assigns Arjun a readmission risk score of 0.84 — very high.
This score doesn’t mean he will be readmitted.
It means: If we don’t intervene, the odds are dangerously high that he will.
What the Model Enables:
A system using this model could trigger an alert before discharge:
“High Readmission Risk: Recommend case manager follow-up within 48 hours.”
That’s it.
One signal.
One conversation.
Potentially one avoided readmission.
Why Trust AI?
Unlike rule-based systems that rely on fixed thresholds (like “age over 65” or “3+ comorbidities”), our model learns from real outcomes. It weighs patterns that doctors may not have time to notice under pressure — like how a certain combo of medications and readmission history is more telling than either factor alone.
This doesn’t replace clinical judgment. It augments it. Think of it as a second opinion — one that’s read 100,000 patient journeys and remembers them all.
In our next section, we’ll look at what happens when hospitals actually act on these insights — and the real-world results when AI is trusted to nudge care forward.

When Hospitals Listen: Real Impact Stories
Imagine a hospital where the readmission alerts aren’t just warnings but triggers for coordinated action. Where care teams get a heads-up before patients like Arjun slip through the cracks. That’s not sci-fi — it’s happening now.
Case Study: Mount Sinai Health System
Mount Sinai Hospital implemented the Heart Health Program, a digital health monitoring initiative aimed at reducing 30-day readmissions for heart failure (HF) patients. The program utilized the RxUniverse platform to prescribe digital care pathways, including the HealthPROMISE digital therapeutic and iHealth mobile apps, to patients’ personal smartphones. These tools enabled remote monitoring of vital signs, such as blood pressure and weight, with data transmitted to care teams for timely interventions.
Key Outcomes:
30-day readmission rate: 10% among program participants, compared to Mount Sinai’s average of approximately 23% and the national average of around 25%. [source]
Global Examples:
- Ng Teng Fong General Hospital in Singapore implemented a real-time risk scoring system to predict 30-day readmissions. This approach successfully reduced the 30-day readmission rate for patients admitted to the medicine department from 11.7% in 2017 to 10.1% in 2019. [source]
- In the UK, the Onward Care program, developed in collaboration with Buckinghamshire Healthcare NHS Trust, utilized AI-enabled sensors in household appliances to monitor recently discharged patients. This initiative led to a 77% reduction in unplanned readmissions among frail patients over a 12-week period. [source]
Human in the loop:
Technology alone doesn’t solve readmissions. It’s the combination of AI insights + clinical judgment + patient-centered care that makes the difference.
For patients like Arjun, this means:
- Personalized follow-up plans
- Timely home health visits or telehealth check-ins
- Medication reviews and social support interventions
In the next and final section, we’ll explore what this all means for healthcare providers — and how companies like ours can partner to bring these solutions to life.

From Proof of Concept to Real-World Change
Arjun’s story is a snapshot of a much larger opportunity. Hospitals around the world face mounting pressures—from rising patient loads to shrinking budgets. Yet, at the same time, they are sitting on a treasure trove of data waiting to be transformed into actionable insights.
Our journey with predictive models shows that the technology is no longer just theoretical. It can be built, tested, and integrated with existing healthcare workflows to deliver real impact. The key lies in collaboration — between data scientists, clinicians, administrators, and technology partners.
What’s Next?
- Scalable Deployment: Moving from proof of concept to hospital-wide deployment requires robust data pipelines, clinician training, and continuous model monitoring to ensure fairness and accuracy.
- Expanding Use Cases: Beyond readmission, predictive models can forecast emergency visits, medication non-adherence, or even identify patients at risk for chronic disease progression.
- Ethical AI in Healthcare: Ensuring transparency, patient privacy, and bias mitigation are essential as AI becomes more deeply embedded in care.
- Partnership Opportunities: We’re eager to collaborate with hospitals, clinics, and healthcare innovators to tailor AI-driven solutions that meet their unique challenges.
Join Us in Shaping Healthcare’s Future
The promise of AI in healthcare isn’t just about algorithms; it’s about changing patient lives. If you’re a healthcare provider seeking smarter tools, a tech enthusiast passionate about medical AI, or an investor interested in transformative health tech — let’s talk.
Together, we can ensure stories like Arjun’s become fewer and farther between.
References
- National Library of Medicine: “All-cause 30-day readmission rates for congestive heart failure”
- Wikipedia: “Heart_failure”
- Pharmmdlive: “Hospital Readmissions: Reducing Costs with Innovative Solutions”
- National Library of Medicine: “Medicare’s Hospital Readmission Reduction Program in …”
- Statista: “Number of hospitals in U.S. that Medicare punished in FY 2023 for high readmission”
- Adelaideaz: “Adelaide Score AI for hospital patient flow a hope to ease South Australia …”
- Nature: “Clinical characteristics and risk factors of preventable hospital readmissions within …”
- POLS one: “Man vs. machine: Predicting hospital bed demand from an emergency department”
- National Library of Medicine: “Impact on Readmission Reduction Among Heart Failure …”
- National Library of Medicine: “Effect of a Real-Time Risk Score on 30-day Readmission …”
- Miicare: “AI kettles and refrigerators contribute to a reduction in hospital readmissions during …”
Enhance Your AI & ML Skills
Struggling to understand concepts like machine learning, neural networks, or generative AI? Dive deeper into the world of AI with expert-led courses on CloudxLab — your gateway to mastering applied AI for the real world.
Visit CloudxLab